

April 2025
An algorithmic challenge – appropriate or inappropriate shock?
Daniel Hinchliffe, Clinical Scientist (Invasive Cardiology), Leeds Teaching Hospitals Trust
Disclosure: The author has no conflict of interests to declare.
Background
A 62-year-old male had a dual chamber ICD (Abbott Gallant) implanted for probable Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC). He contacted the pacing department with symptoms of breathlessness when walking up a hill and mentioned that he thought he might have received a shock.
The device detection parameters were as follows:
- VT-1 Monitor Zone 130bpm
- VT-2: 187bpm, 30 intervals with ATP & shocks
- VF: 230bpm, 16 intervals with ATP whilst charging and shocks
- SVT discrimination dual chamber on.
Below is the EGM that was sent via remote monitoring.
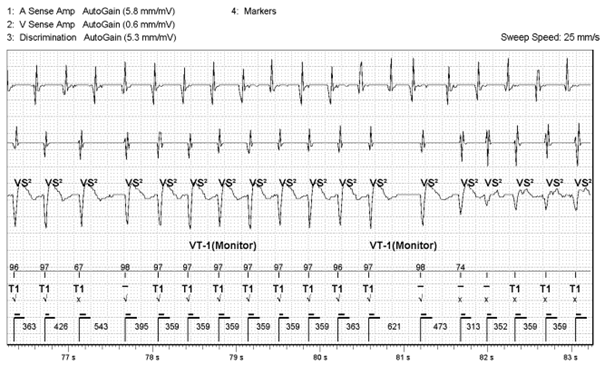
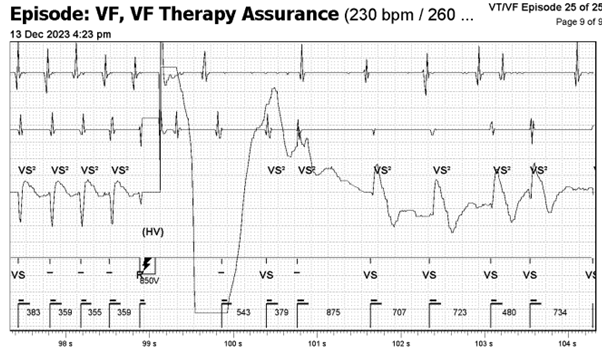
Figure 1: Stored EGM
QUESTION 1
What is the arrhythmia?
QUESTION 2
What information would you want to ensure diagnostic certainty?
QUESTION 3
Has the shock been delivered appropriately?
QUESTION 4
What arrhythmia is present in this change in morphology (and what is the supporting evidence for and against these possibilities and what further information would help?)
Answer
Unsure, can’t be certain
- The fact that the cycle length remains essentially the same would strongly support this being aberrant conduction of AT assuming the initial arrhythmia was AT with rapid ventricular response. A less common ‘fooler’ for this is a different exit in an inner loop VT. N.B. Inner loop VTs are reentrant cirucuits ‘protected’ within a scar that can have multiple exits from the scar giving different VT morphologies as the exits change but often without noticable change to cycle length as the inner loop circuit remains constant.
- The first beat of the clearly changed morphology is also unusual as it comes in at a cycle length shorter than the normal proposed AV conduction would allow (313 vs 359ms) and this wouldn’t generally happen with bundle branch block. This adds less support to the aberrant hypothesis.
- The beat before this short coupled beat appears now to be fusion between the 2 morphologies. This could represent VT fusing with conducted AT. Or perhaps there could be a single PVC fusing with conducted AT that conceals in the right or left bundle branch setting up aberrant conduction. It is unclear from the tracing.
- At the end, the shock ‘corrects’ both A and V channels so that doesnt help distinguish. Ongoing AT with a cardioverted V channel would have supported VT, as would ongoing VT with a cardioverted A channel.
As such, the cause of this temporary morphology and amplitude change remains uncertain.
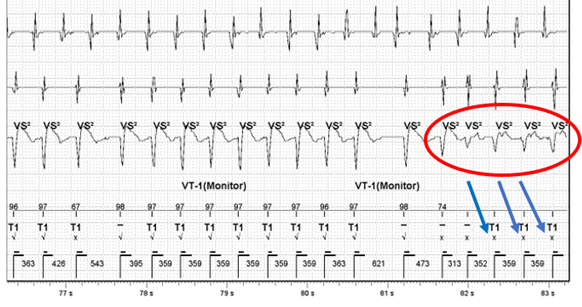
Figure 2: Signal change with morphology mismatching
QUESTION 5
What algorithm is triggered leading to a shock?
Answer
VFTA – Ventricular Fibrillation Therapy Assurance
Ventricular Fibrillation Therapy Assurance (VFTA) works in the background when the first fast interval average is detected, and will check the VFTA counter at 5 different points during the episode in the far-field sensing channel. VFTA was triggered due to the low amplitude counter which resulted in the VF zone being lowered to the lowest active treatment zone +100ms – i.e. 400ms. Six ‘VF’ markers are required to trigger VF therapy due to the VFTA algorithm dropping the number of intervals for detection (NID) from the programmed sixteen. Dropping the NID from sixteen to six accelerates time to therapy but the downfall of this is clear in the current EGM, whether this represents abberancy or non-sustained VT in rapidly conducted AT. VTFA only uses two independent counters; a low amplitude counter and a pause counter. The change in amplitude and morphology activated the low amplitude counter as at least two of the beats (circled in red) had signals measuring between 0.3 – 0.6mV. This triggered VFTA which caused the device to start charging due to satisfying the NID criteria of six (Figure 3, circled in red). This leads to an inappropriate shock for the patient but is algorithmically correct device function.
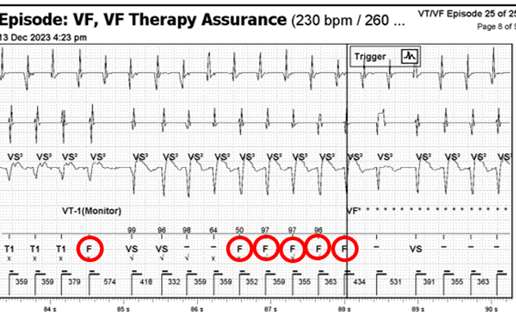
Figure 3: F markers causing device to start charging
VFTA is an algorithm that identifies polymorphic VT/VF that is at risk of being under-sensed. It does this by assessing sensing on the discrimination channel when a ventricular event is ongoing.
The algorithm works by using two independent counters, and is triggered when either one is true. A low amplitude counter looks for consistently small signals (0.3 – 0.6mV) and increments the counter by one. This triggers if the counter is >2. Large signals (>0.6mV) resets the counter to zero. The pause counter looks for signal dropout, which is defined as no sensing present. Two seconds without a VS2, increments the counter by one and large signals (>1mV) with a VS2 resets the counter to zero. This triggers if the pause counter in >1. Once VFTA is triggered a number of parameters are changed:
1) Detection is switched to single therapy zone – VF only
2) New VF detection rate is decreased to the lowest programmed active therapy zone + 100ms (400ms max)
3) Number of intervals to detection is decreased to 6
4) End of episode (previously Return to Sinus) is increased to 7 intervals
5) Permanently programmed VF zone therapies are used
VFTA has been evaluated retrospectively on >500,000 EGMs from 20,000 devices with the results highlighting that the algorithm altered high voltage therapy in 0.34% (67/20,000) of devices with an 81.9% episode positive predictive value and 79.1% true positive rate. VFTA delivered high voltage therapy to 0.22% (44/20,000) of the devices that experienced at least one potentially undertreated VT episode (Wilkoff et al, 2022). Overall, the results of Wilkoff’s study were positive in that the VFTA algorithm delivered high voltage therapy to 86% of patients who would have otherwise been untreated for potentially life-threatening arrhythmias. However, it must be appreciated that the validation used derived data as opposed to real-world prospective data and therefore might lack the rigour associated with prospective clinical trials.
A noticeable finding that warrants recognition includes the fact that a small number of patients would have received inappropriate therapy (0.07%, 14/20,000) if VFTA was programmed on due to noise oversensing (4), physiological oversensing (4), and SVT (6)However, this can be mitigated with appropriate discriminator programming in most cases as suggested by Stroobandt and colleagues (2019).
Although the current patient received an inappropriate shock, the benefits far outweigh the risk as evidenced by Wilkoff’s validation study as well as a handful of case reports that demonstrate the effectiveness of the algorithm (Bera et al, 2022; Brignoli et al, 2023). It is crucial for the Physiologist/Healthcare Scientist to recognise inappropriate device therapy and to make a clinical decision on next steps for device programming as well as seeking advice if needed.
References:
- Bera, D., Mani, S., Sen, R., Majumder, S., Halder, A. and Ray, A. (2022) Inappropriate ventricular fibrillation annotation and defibrillator discharge despite the same tachycardia cycle length in ventricular tachycardia-1 zone in an Abbott defibrillator – What is the mechanism? Pacing and Clinical Electrophysiology. 46 (2), pp. 169-171.
- Brignoli, M., Mattera, A., Chianese, R., Simonette, A., Vittoria, D. and Viscusi, M. (2023) Real-world use of a novel ventricular tachycarrhythmia detection algorithm: A case report. Heart Rhythm. 9 (12), pp. 929-934.
- Stroobandt, R.X., Duytschaever, M.F., Strisciuglio, T., Heuverswyn, F.E.V., Timmers, L., De Pooter, J., Knecht, S., Vandekerckhove, Y.R., Kucher, A. and Tavernier, R.H. (2019) Failire to detect life-threatening arrhythmias in ICDs using single-chamber detection criteria. Pacing and Clinical Electrophysiology. 42 (6), pp. 583-594.
- Wilkoff, B.L., Sterns, L.D., Katcher, M.S., Upadhyay, G., Seizer, P., Kang, C., Rhude, J., Davis, K.J. and Fischer, A. (2022) Novel ventricular tachyarrhythmia detection enhancement detects undertreated life-threatening arrhythmias. Heart Rhythm 02. 3 (1), pp. 70-78.
NOTE: Edited by Simon Modi. All cases are reviewed for accuracy, but if you have concerns, please direct them via the contact form on the website.
Disclaimer: The British Heart Rhythm Society (BHRS) collates submissions for the ECG/EGM challenge on this website. These submissions, along with any accompanying answers, are provided by external contributors and are published for informational purposes only. BHRS does not endorse, guarantee, or warrant the accuracy, completeness, or reliability of any submissions or answers provided.
Leave A Comment
You must be logged in to post a comment.